




FAQs
The Epilepsy Range
When should I measure serum phenobarbital concentrations? (Timing/Peak/Trough samples)
If STARTING phenobarbital or CHANGING DOSE:
Ideally, perform a full haematology and Biochemistry including bile acid stimulation test prior to initiating phenobarbital therapy to obtain baseline values and confirm drug suitability.
Initially, check serum phenobarbital (PB) levels at 2-3 weeks, then 3 months post starting/dose changes, then every 6-12 months as routine for stable patients.
TIMING of blood sample:
It is not necessarily the timing of sampling that is important, but more consistency. i.e. the same time of day each time, and maintaining consistency for that patient. There will be small daily fluctuations, but in most patients these are not clinically relevant and measuring at the same time of day each time will help to eliminate any daily fluctuation, confusing results after a dose change.
The only situations where it is advisable to check peak or trough samples are as follows:
– If the patient is close to the upper reference range (e.g. close to 35mg/L) and we want to make sure the patient stays below this threshold: Peak sample: 4-6 hours post pill
– If the patient is experiencing breakthrough seizures or at the low end of the therapeutic window, and we want to know how low the serum concentration goes/is the serum concentration sub-therapeutic, and a dose increase is required: Trough samples: Just before the next pill is dosed, so ~10-12 hours post pill
Haematology and biochemistry + BAST every 6-12 months alongside serum PB in stable patients. More frequent screening is advised if concerned or unstable patient with poor seizure control.
What is autoinduction?
Phenobarbital induces liver enzymes i.e. it increases their activity. Hence the increased ALP, ALT and GGT values often seen on blood samples. This also increases the metabolism of the phenobarbital itself. This results in decreases in serum PB concentration over time. Re-evaluation of serum PB concentration is therefore recommended at 3 months and then every 6-12 months (or more frequently in unstable patients).
Why is it advised not to change the diet of patients on Vetbromide?
As per Vetbromide’s SPC ‘The salt content of a dog’s diet during the treatment period should be maintained at a stable level. It is advisable not to change the dog’s diet during therapy.’ and ‘Where possible, the diet of treated dogs should therefore not be altered. Seek veterinary advice before making any change to the dog’s diet’
This is because bromide ions directly compete with chloride ions for renal tubular reabsorption, and the relationship between dietary salt and serum bromide concentrations is inversely proportional:
A high salt diet = lowers bromide concentrations = increased risk of seizures.
A low salt diet = increased bromide concentrations = increased risk of side effects/bromotoxicosis.
If a dietary change is required, this must be done gradually, minimising changes to the overall salt content where possible. The IVETF guidelines advises dietary changes should be made over at least 5 days, and serum potassium bromide concentrations should be monitored following dietary changes, especially if the dog experiences adverse events or has unexpected seizures.
When should I start anti-epileptic drug (AED) therapy?
The following recommendations come from the International Veterinary Epilepsy Task Force (IVETF) consensus proposal: medical treatment of canine epilepsy in Europe. Bhatti et al. BMC Veterinary Research (2015)
The IVETF consists of multiple world-leading neurologists, who have deemed it advisable to commence AED treatment when the patient experiences ≥ 2 unprovoked (ie. non-reactive) seizures, ≥ 24 hours apart in a ≤ 6 month period. This consensus is detailed in their ‘Medical treatment of canine epilepsy in Europe’ statement.
It is important to try to reduce or stop seizures altogether, as each time a seizure occurs, it can cause wider damage to cells in the brain and can increase the likelihood of more seizures occurring – a phenomenon known as ‘kindling’.
Extract from IVETF medical treatment of canine epilepsy in Europe:
“In people, clear proof exists that there is no benefit in initiating AED treatment after a single unprovoked seizure, but there is evidence to support starting treatment after the second seizure. In dogs, long-term seizure management is thought to be most successful when appropriate AED therapy is started early in the course of the disease, especially in dogs with a high seizure density and in dog breeds known to suffer from a severe form of epilepsy.”
The authors recommend initiation of longterm treatment in dogs with idiopathic epilepsy when any one of the following criteria is present:
• Interictal period of ≤ 6 months (i.e. 2 or more epileptic seizures within a 6 month period)
• Status epilepticus or cluster seizures
• The postictal signs are considered especially severe (e.g. aggression, blindness) or last longer than 24 hours
• The epileptic seizure frequency +/or duration is increasing +/or seizure severity is deteriorating over 3 interictal periods
What do I do if the patient has high liver values (ALP/ALT/GGT/AST) whilst on phenobarbital?
As per the Soliphen SPC: “Phenobarbital may increase the activity of serum alkaline phosphatase and transaminases. These may demonstrate non-pathological changes, but could also represent hepatotoxicity, so liver function tests are recommended. Increased liver enzyme values may not always require a dose reduction of phenobarbital if the serum bile acids are in the normal range.”
In practice:
• Most dogs will experience an increase in liver parameters due to hepatic microsomal enzyme induction whilst receiving phenobarbital, most often without actual hepatotoxicity. We most commonly see this affecting the patients’ ALP, but to a lesser extent ALT and GGT.
• Whilst most dogs experience an increase in ALP around 3-5 times the upper reference range, it is not uncommon to see patients with higher values than that, and the value itself is not a reason to worry or to cease Soliphen treatment
• It is important to look at the whole clinical picture, including any other clinical signs the patient may have and other liver parameters.
• AST can be a very useful measure as it is not affected by phenobarbital enzyme induction and therefore, we expect this to be normal in the absence of hepatotoxicity. If the AST is also elevated, this may raise suspicion of an underlying liver problem and warrants further investigation.
• The serum concentration of Phenobarbital is also useful to assess, as generally true hepatotoxicity is seen with serum concentrations persistently over 35mg/L or at daily doses exceeding 20mg/kg/day.
• A bile acid stimulation test is recommended to assess liver function – even despite high ALP, ALT or GGT, we would expect the BAST to be normal.
• It is worth considering further liver investigations e.g. ultrasound or advanced imaging as appropriate
• It is prudent to rule out other causes of increased ALP e.g. steroid use (topical or oral) and possible Cushings disease
• If the BAST is normal, the patient is well and other causes of ALP increases are ruled out, then it is recommended to continue to simply monitor the patient’s liver values every 3-6 months. Most dogs will plateau at a certain level, but some may keep rising. Of course, this plan should be modified if the patient becomes unwell at any point.
• If the BAST is abnormal, if the AST is elevated or if there are clinical signs then we need to try and ascertain is it: a) due to Soliphen itself and therefore requires Soliphen withdrawal, or b) is not due to Soliphen e.g. neoplasia, hepatitis/cholangitis, pancreatitis etc, where further investigations should be conducted before Soliphen withdrawal if possible. If the cause is not directly related to phenobarbital, Soliphen may still require withdrawal, as it is a contraindication to use PB in patients with severe liver insufficiency. If the liver disease is mild, expected to be short-lived or can otherwise be treated, then it may be possible to continue Soliphen/PB for the sake of the patient’s continued seizure control.
Any increases in liver enzymes, even if not considered pathological/considered normal for PB, should still be reported as a PV complaint.
Which anti-epileptic drug should I choose?
The 2015 ACVIM Small Animal Consensus Statement on Seizure Management in Dogs provides evidence-based levels of recommendations to guide clinicians in choosing appropriate anti-epileptic drug therapy for dogs. Although now over 10 years old, the recommendations are still valid today.
They recommend the following:
First line recommendation: Phenobarbital or Imepitoin
Second line recommendation: Potassium bromide (first line in patients with liver insufficiency)
Third line recommendation: Levetiracetam
Fourth line and lower: Zonisamide and other infrequently used AEDs.
Access the consensus statement here: https://pmc.ncbi.nlm.nih.gov/articles/PMC4913615/pdf/JVIM-30-477.pdf
How effective are phenobarbital and potassium bromide?
Phenobarbital remains the first-line recommended anti-epileptic agent. According to the International Veterinary Epilepsy Task Force (IVETF) consensus statement (2015) phenobarbital seems to be effective in decreasing seizure frequency in up to 93 % of dogs with idiopathic epilepsy when plasma concentrations are maintained within the therapeutic range of 25−35 mg/L. According to Charalambous et al. (2014) [17], there is overall good evidence for recommending the use of PB as a monotherapy AED in dogs with idiopathic epilepsy.
Potassium Bromide is considered effective as an initial therapy in dogs, achieving seizure remission in over 50% dogs with an overall improvement in 74% of dogs as monotherapy (Boothe et al 2012). Thus, it provides a suitable alternative to first-line medication in patients with liver insufficiency. It is also a recommended ACVIM 2nd line anti-epileptic agent with up to 83% of dogs with refractory epilepsy improving with potassium bromide as an adjunct to phenobarbital (Podell 1993).
What is the shelf life of Soliphen?
As per the SPC:
Shelf life of the veterinary medicinal product as packaged for sale: 3 years
Do not store above 25°C. Any remaining portions of divided tablets should be replaced in the blister pocket, and the blister strip should be returned to the cardboard box. Any tablet portions remaining after 3 days should be discarded.
Note: The Soliphen 15mg and 120mg SPC states that remaining tablet portions should be given at the next administration.
What are the ideal therapeutic serum levels for potassium bromide/Vetbromide?
As per the Vetbromide SPC, the ideal serum concentrations are:
1,000-3,000mg/L when used as monotherapy
800 – 2,000mg/L when used as adjunct therapy.
If the clinical response is not satisfactory or if adverse reactions occur, the dose may be adjusted based on the dog’s serum bromide levels. Serum concentrations should be measured after each dose adjustment once steady-state serum levels have been reached (typically 3 months after a change), unless earlier evaluation is necessary. Long-term monitoring of serum bromide concentrations should be performed as clinically justified by the individual case.
As the therapeutic and safety range for potassium bromide is very wide, and there is a lot of individual variability in tolerance, unlike phenobarbital, it is acceptable for patients to have higher serum concentrations than those listed, so long as the patient does not experience adverse events.
When is the steady-state serum concentration achieved with Vetbromide?
As per the Vetbromide SPC:
It takes ~3 months to achieve steady-state serum concentrations when started on maintenance dosing (15mg/kg BID adjunct, 30mg/kg BID monotherapy).
This can be achieved sooner with loading (see related FAQ).
This is because the half-life of potassium bromide is very long (14-40days).
Therefore, it is advisable to wait 3 months before measuring serum concentrations after starting or any dose change. If Vetbromide has been loaded, this can be done after 1 week.
What are the ideal therapeutic serum levels for phenobarbital/Soliphen?
As per the Soliphen SPC: typically concentrations of 15-40 μg/ml (=mg/L) are effective in controlling epilepsy.
This is also often the reference range stated on laboratory results.
However, the International Veterinary epilepsy task force (2015) and the 2015 ACVIM Consensus Statement on canine epilepsy advise that most patients are well controlled between 25-30mg/L and that hepatotoxicity is more likely to develop when serum concentrations are persistently >35mg/L. Therefore, in practice, these recommendations are usually advised as the ideal and top-end ranges.
When is steady-state serum concentration achieved with Soliphen?
As per the Soliphen SPC:
Steady-state serum concentrations are not reached until 1-2 weeks after treatment is initiated. The full effect of the medication does not appear for two weeks, and doses should not be increased during this time.
Therefore, it is advisable to wait at least 2 weeks before measuring serum concentrations after initiating therapy or any dose changes.
What is the shelf life of Vetbromide?
As per the SPC:
Shelf life of the veterinary medicinal product as packaged for sale: 4 years
Store below 30 °C. After piercing a blister, replace unused tablet parts into the blister and place the blister back into the carton. Remaining tablet portions should be given at the next administration
How is Vetbromide synergistic with Soliphen?
Phenobarbital acts on GABA receptors and opens the GABA channel, where GABA is the principal inhibitory neurotransmitter. GABA receptors are chloride ion channels; therefore, opening the channel allows more negatively charged Cl ions into the cell. This hyperpolarises the neurone, meaning the neurone is harder to fire.
Bromide travels through chloride ion channels – including GABA. Bromide ions are smaller than chloride therefore diffuse through at a quicker rate. Therefore, phenobarbital opens the GABA channel for the bromide ions to pass – this is how they work synergistically.
How do I load Vetbromide? What are the loading doses?
The loading protocol as per Vetbromide’s SPC:
-60mg/kg BID for 5 days (120mg/kg per day) -then follow on with maintenance dosing regime.
-Patients may benefit from being hospitalised for the first 48 hours to monitor for AE’s and for those who are outpatients, daily telephone contact is recommended (IVETF guidelines).
Note: Other loading dosing protocols exist, and can vary widely in dosing regimens. These would be considered ‘off-license’ for Vetbromide. If you are considering an alternative loading regimen, we advise discussing the case with our technical team or with a neurospecialist.
How to convert the serum phenobarbital concentration between mg/L and umol/L?
The conversion factor from mg / L (same as μg / ml ) to μmol / L is a multiplication by 4.306
e.g. 35mg/L x 4.306 = 150.71umol/L PB
Therefore, to convert from μmol / L to mg / L you divide by 4.306
e.g. 150umol/L÷ 4.306 = 34.8mg/L
The ideal range of 25 – 30mg/L equates to ~107 – 130umol/L
And 35mg/L therefore equates to ~150umol/L
The Anxiety Range
What is the dose of Fluoxevet®? Onset of effect?
Fluoxevet® should be administered orally at a once daily dose of 1 to 2 mg/kg bodyweight. Tablets can be divided into 2 or 4 equal parts to ensure accurate dosing. Clinical improvement with Fluoxevet is expected within 1 to 2 weeks, but may take longer. Clinical studies have shown that a beneficial response has been demonstrated for up to 8 weeks treatment with fluoxetine. The tablets may be given with or without food.
Can Fluoxevet® be administered with food?
Fluoxevet® can be administered with or without food.
Is Fluoxevet® flavoured?
Fluoxevet® is flavoured with a beef flavouring and masking agent. Fluoxevet® contains no ingredients of animal origin or gluten.
Why should you switch to Fluoxevet®?
Fluoxevet® offers accurate and flexible dosing in a single 32mg double-divisible tablet with a unique flavour to improve compliance. It has a 120-day open shelf life (4 years unopened) and is cost-effective. When switching from a licensed veterinary fluoxetine to Fluoxevet®, a mg to mg switch can be made at the next dose.
What are the storage requirements of Fluoxevet®?
Fluoxevet® has an unopened shelf life of 4 years and a shelf life of 120 days after opening. Any unused portions of divided tablets should be returned to the bottle, which should then be placed back in the cardboard box.
Should you taper the dose of Fluoxevet® at the end of treatment?
According to the Fluoxevet® SPC (section 3.9 Administration routes and dosages), at the end of treatment, it is not necessary to taper or reduce doses because of the long half-life of this veterinary medicinal product.
Are there any medications that should not be used in combination with Fluoxevet®?
Fluoxevet® should not be given concomitantly with veterinary medicinal products that lower the seizure threshold (e.g. phenothiazines such as acepromazine or chlorpromazine). Do not use the product in conjunction with other serotonergic agents (e.g. sertraline) and monoamine oxidase inhibitors (MAOIs) [e.g., selegiline hydrochloride (L-deprenyl), amitraz] or tricyclic amines (TCAs) (e.g. amitriptyline and clomipramine).
A 6-week washout interval should be observed following discontinuation of therapy with Fluoxevet® prior to the administration of any veterinary medicinal product that may adversely interact with fluoxetine or its metabolite, norfluoxetine. Additionally, fluoxetine is largely metabolised by the P-450 enzyme system, although the precise isoform in dogs is unknown. Therefore, fluoxetine should be used with caution with other veterinary medicinal products.
What is the dose of Sileo®? Onset/duration of effect?
The Sileo® dose is 125 mcg/m². It should be administered onto the oral mucosa between the dog’s cheek and gum.
If the calculated dose is greater than 6 dots, the dose should be divided between both sides of the mouth. The onset of Sileo’s® effect is typically 30–60 minutes, and lasts approximately 2–3 hours.
Can Sileo® be administered with food?
If Sileo® is swallowed, it will become ineffective. Therefore, feeding the dog or giving it treats within 15 minutes after administration of the oromucosal gel should be avoided. In case the gel is swallowed, the dog can be given another dose if necessary 2 hours after the previous dose.
What are the storage requirements of Sileo®?
Sileo® has a shelf life of 3 years. Once opened, Sileo® has a shelf life of 4 weeks. Store at room temperature. As Sileo® is sensitive to light, it should be recapped and stored in its original box.
How often can Sileo® be administered?
Sileo® can be administered up to 5 times per noise event, with a minimum interval of 2 hours between doses, only if the noise continues and the dog’s signs reappear. If the dog remains calm, additional doses are not required.
How does Sileo® differ from injectable dexmedetomidine?
Although Sileo® and injectable dexmedetomidine contain the same active ingredient, their effects differ due to the route of administration. Sileo® is administered oromucosally, which limits the bioavailability of dexmedetomidine to approximately 28%, meaning only about one-quarter of the dose is systemically absorbed. At this lower plasma concentration, studies show that Sileo® produces a calming (anxiolytic) effect without sedation, with minimal systemic effects.
Is Sileo® flavoured?
Sileo® contains no flavouring agent and is odourless (to humans). The absence of flavouring is intentional, as Sileo® should not be swallowed but administered oromucosally. Sileo® does not contain any animal-derived amino acids, nor any carbohydrate from grains.
What is the dose of Tessie®? Onset/duration of effect?
Tessie® is administered orally at a dose of 0.1 ml/kg bodyweight (equivalent to 30 ug/kg or 1 ml per 10 kg). Please refer to the pictograms within the datasheet for advice on correct administration. It is advised not to feed the dog for one hour before to one hour after treatment. A small treat can be given to ensure that the dog swallows the solution. Water can be freely available.
For anxiety or fear triggered by noise, the first dose should be given one hour before a known anxiety-inducing stimulus, at the first signs of anxiety, or when the owner detects a typical triggering event, such as fireworks.
For anxiety or fear triggered by owner departure, the dose should be administered one hour before the expected departure.
The onset of effect is usually seen within 30 minutes to 1 hour. Tessie® is expected to provide at least three hours of effect; if the fear-triggering event continues and signs of anxiety reappear, Tessie® may be redosed after 3 hours, with a maximum of three doses in 24 hours, for up to nine consecutive days.
Can Tessie® be administered with food?
According to the Tessie® SPC, section 4.9, do not feed the dog for one hour before to one hour after treatment as absorption may be delayed. A small treat can be given to ensure that the dog swallows the solution (and to make positive associations). Water can be freely available.
Feeding may slow absorption of Tessie® and delay the onset of action.
What are the storage requirements of Tessie®?
Tessie® has a shelf life of 3 years. Once opened, Tessie® has a shelf life of 12 months. The bottle should be stored in a refrigerator, but may be stored for short periods of time at or below 25°C. Keep the bottle in the outer carton in order to protect it from light.
How often can Tessie® be administered?
Tessie® can be dosed up to three times within 24 hours, with at least 3 hours between doses, for a maximum of 9 consecutive days. It is possible to include a break between treatment periods – for example, up to 9 days of dosing, followed by a 1-2 day break, after which a new 9 day course could begin. Given Tessie’s® elimination time of approximately 8.5 hours, the drug would be effectively cleared after a 24-hour break in healthy patients.
Can Tessie® be administered alongside other behaviour-modifying drugs?
According to the Tessie® SPC, section 4.8: The use of other central nervous system depressants may potentiate the effects of tasipimidine, and therefore an appropriate dose adjustment should be made. The safety of tasipimidine in combination with tricyclic antidepressant clomipramine, serotonin reuptake inhibitor fluoxetine, anaesthesia premedications (dexmedetomidine, methadone), induction agents (propofol) and inhalation anaesthetics (isoflurane) has been demonstrated in studies in healthy dogs. When used concomitantly with clomipramine or fluoxetine, the tasipimidine dose should be reduced to 20 μg/kg bodyweight.
Is three hours of effect sufficient for separation-related problems?
Tessie® is expected to last three or more hours.
Typically, separation-related problem behaviours begin at the time of the trigger, for example, when an owner signals an impending departure (even before they actually leave), or shortly after the owner has left. The highest levels of observable distress behaviours usually occur within the first hour. By giving Tessie® one hour before departure, in the ideal case, the entire separation runs more smoothly as the anxiety is not being triggered in the first place. Therefore, the duration of effect is not necessarily directly related to the plasma concentration. For this reason, although owners in the clinical trial were allowed to administer the product up to three times within a 24-hour period, few required more than a single application.
What are the key considerations when prescribing Tessie®?
It is worth noting that the goal of treatment with Tessie® is anxiolysis without clinical sedation, meaning the dog should remain calm but fully functional. For optimal effect, Tessie® should be administered pre-emptively (approx. 1 hour) before the anticipated trigger. In dogs that are already highly aroused, significant noradrenaline release may already have occurred, which may limit Tessie’s® effectiveness. Tessie® should be given without food, as feeding may slow absorption and delay the onset of action. A small treat may be used to encourage swallowing and help create a positive association. Water can be freely available.
What is the difference between Tessie® and Sileo®?
Tessie® can be viewed as an evolution or ‘next generation’ of Sileo®. The main difference is their licensed indications: Tessie® has a dual purpose as it is licensed for situational anxiety triggered by owner departure and noise-related anxiety, whereas Sileo® is licensed only for noise-related anxiety.
Tessie® may offer practical advantages in some cases, including a liquid oral formulation rather than an oromucosal gel, as well as presentation in a larger volume. However, Sileo® may still be preferred in certain cases and can continue to be used where it is considered the most appropriate choice.
Please refer to our Tessie® and Sileo® guide for more information.
Can the dose of Tessie® be reduced?
A test dose of Tessie® should be given before the dog is left alone after treatment. After administering the test dose, observe the dog to ensure the dose is appropriate. If the dog appears drowsy, uncoordinated, or unusually slow to respond to its owner after treatment, the next dose may be reduced by one-third (to 20ug/kg). Any dose adjustment should only be made under veterinary advice.
What is the dose of Bonqat®? Onset/duration of effect?
Bonqat is administered orally as a single dose of 5 mg/kg (0.1 ml/kg) approximately 90 minutes before the stressful event. The effect of the veterinary medicinal product can last approximately 7 hours.
How does Bonqat® work?
Pregabalin binds to the auxiliary subunit (alpha2-delta protein) of voltage-gated calcium channels in the central nervous system thereby reducing the release of various neurotransmitters (glutamate and monoaminergic neurotransmitters) and producing its anxiolytic effect.
Can Bonqat® be administered with food?
Bonqat® can be administered either directly into the mouth or mixed with a small amount of food. Large amounts of food may delay the onset of effect. The small dosing volume and flavoured oral solution will aid with administration. In clinical trials, 79% owners found it easy to give Bonqat® directly into the cat’s mouth, and compliance was good in 95% of cats1.
What are the storage requirements of Bonqat®?
Bonqat® has a shelf life of 3 years. Once opened, Bonqat® has a shelf life of 6 months. The bottle should be stored in a refrigerator but may be stored for short periods of time at or below 25°C. Bonqat® is a schedule III drug.
Does Bonqat® affect the clinical examination?
Similar to gabapentin, pregabalin may influence certain aspects of the clinical exam, so this should be considered during assessment.
In terms of mobility, most cats maintained normal activity levels and were able to stand and walk normally during the clinical trials. There were no clinically relevant changes observed in routine lab parameters. Because pregabalin has analgesic properties, it may influence pain assessment during the exam. In terms of physiological parameters, occasional reductions in body temperature and heart rate were noted, with minor changes in blood pressure, although values generally remained within normal physiological ranges1.
Of course, stress can also affect physiological parameters (such as heart rate, respiratory rate, temperature, blood pressure), and pain scoring.
Can you administer Bonqat® before sedation or anaesthesia?
As Bonqat® is licenced for vet visits, it is likely that some cats could require follow-on sedation or anaesthesia. As the use of other central nervous depressants can potentiate the effects of pregabalin, appropriate dose adjustments should be made. The decision to use Bonqat® before sedation or anaesthesia should be based on a risk:benefit assessment adapted to each individual patient. In the clinical trial, seven cats in the Bonqat® group (fourteen in the placebo group) required sedation with no issues reported. The clinical study for Bonqat® is open access1.
How does Bonqat® differ from gabapentin?
As the licensed anxiolytic for cats, Bonqat® is the most appropriate option and should be considered first according to the prescribing cascade.
It is difficult to accurately compare the clinical effects of pregabalin and gabapentin, as gabapentin is used at varying doses (50–200 mg per cat, often with additional doses 12 hours before) and its effects are dose-dependent, meaning the expected clinical response may differ. Since both gabapentinoids share the same mechanism of action, we would expect them to have similar effects, including both therapeutic benefits and potential adverse events. From a practical standpoint, pregabalin is more potent than gabapentin, requiring a lower dose. It also has a longer duration of effect (half-life of ~14 hours vs. ~3–4 hours) and a faster onset of action (1.5 hours vs. 2–3 hours). In humans, pregabalin is absorbed more quickly, and its absorption is linear, whereas gabapentin’s absorption becomes saturated at higher doses ie. the bioavailability decreases. As Bonqat® is available as a flavoured oral liquid at a dose of 5 mg/kg, while gabapentin dosing and formulations can vary, this may allow for more accurate dosing and potentially more predictable effects.
Can Bonqat® be prescribed without seeing the cat?
The decision to prescribe Bonqat® without seeing the cat will be case dependent and should be based on a risk:benefit assessment by the prescribing clinician. In the interest of animal welfare, prescription of Bonqat® could be justified, and this should be documented within the patient’s clinical notes.
We refer you to the under-care guidance provided by the RCVS.
The Anti-Tox Range
What is the dose of Ziapam®? Onset of effect?
For administration by slow, intravenous injection only. In dogs and cats:
– Short-term management of convulsive disorders: 0.5mg/kg bw (equivalent to 0.5 ml/5kg). Given as a bolus and may be repeated up to 3 times, at ≥10-minute intervals.
– Short-term management of skeletal muscle spasm: 0.5-2.0 mg/kg bw (equivalent to 0.5-2.0 ml/5kg).
– As part of sedation protocol: 0.2-0.6 mg/kg bodyweight (equivalent to 0.2-0.6 ml/5kg).
– As part of pre-anaesthesia protocol: 0.1-0.2 mg/kg bodyweight (equivalent to 0.1-0.2 ml/5kg).
What are the storage requirements of Ziapam®?
Ziapam® solution for injection has an unopened shelf life of 4 years and should be used immediately after opening. Any solution remaining in the ampoule following withdrawal of the required dose should be discarded. Store in the original package, at 25°C and protected from light. Diazepam is a schedule IV controlled drug.
Is Ziapam® formulated as a water-based solution, an emulsion, or an oil-based product?
Ziapam® 5mg/ml is solution for injection – see below for list of excipients.
Active substance:
Diazepam
Excipients:
Benzyl alcohol (E1519)
Benzoic acid (E210)
Sodium benzoate (E211)
Propylene Glycol
Ethanol (96 per cent)
Sodium hydroxide (for pH adjustment)
Water for injection
Can Carbodote® be administered with food?
Carbodote® is intended to be administered on an empty stomach where possible, as this optimises its adsorptive capacity. As per the Carbodote® package insert, we recommend leaving an interval of ideally three hours between meals and/or medications and the administration of activated charcoal, in order to minimise any potential impact on their efficacy. That said, due to the high adsorptive capacity of Carbodote®, it is unlikely that a small meal would significantly affect its efficacy. There may be situations where activated charcoal needs to be given with food to ensure safe or practical administration (e.g. in a poorly compliant patient).
What are the storage requirements of Carbodote®?
Carbodote® Gels have an unopened shelf life of 4 years and a shelf life of 1 month after opening. Carbodote® Liquid has a shelf life of 2 months after opening. Store at room temperature and keep in a cool, dry place away from heat sources and direct sunlight.
How often should Carbodote® be administered?
For substances that persist in the body, Carbodote® Repeat or Carbodote® Liquid may be administered every 4–6 hours for 24–48 hours.
Please refer to our activated charcoal guideline for more information.
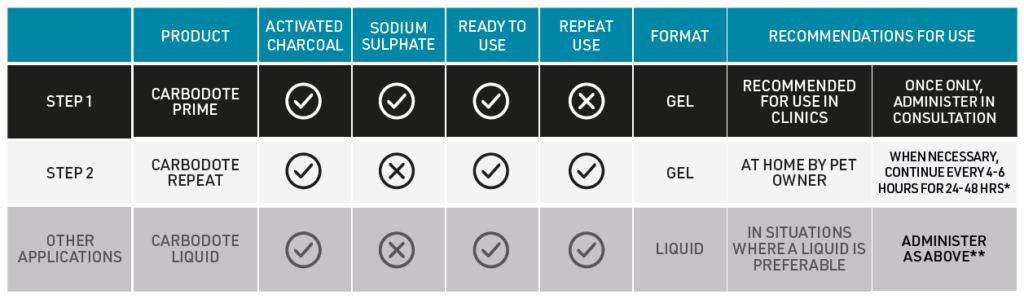
What is the difference between Carbodote® Prime, Carbodote® Repeat and Carbodote® Liquid?
The Carbodote® range includes three activated charcoal products:
Carbodote® Prime – 30% activated charcoal gel syringe with sodium sulphate to speed gastrointestinal transit. Use it first and only once.
Carbodote® Repeat – 30% activated charcoal gel syringe without sodium sulphate, suitable for repeat administration when needed.
Carbodote® Liquid – 20% liquid activated charcoal formulation in 100 ml bottles for when a liquid preparation is preferred. Contains activated charcoal only and can be repeated where required.
The following table summarises the key differences
What is the recommended volume of Carbodote®?
Carbodote® Prime and Carbodote® Repeat syringes contain 60ml of Carbodote® (30% activated charcoal), which treats a 20 kg patient.
Carbodote® Liquid contains 100 ml of Carbodote® (20% activated charcoal), which treats a 20 kg patient.
It is recommended to administer at least 1g/kg activated charcoal. This equates to:
– 3ml/kg (1 dot per 2 kg) of Carbodote® Prime or Repeat
– 5ml/kg of Carbodote® Liquid.
Which species can Carbodote® be administered to?
Carbodote® Repeat and Carbodote® Liquid are indicated for dogs, cats and exotic pets. Carbodote® Prime is indicated for dogs and cats only.
Are Carbodote® syringes recyclable?
Yes, Carbodote® syringes are recyclable, once empty, of course! The syringe is made of PET.
What is the dose of Vitamivet K1® injectable and tablets?
Intravenous treatment: The recommended dose is 5 mg/kg (equivalent to 0.5 ml/kg body weight) administered by slow intravenous injection, prior to initiating oral therapy. If oral treatment cannot be started promptly, the intravenous dose may be repeated once after 12–18 hours.
Oral treatment: The recommended dose is 5 mg/kg body weight once daily (equivalent to 1 tablet per 10 kg body weight) for 21 days, or longer if required. Tablets can be divided into halves or quarters to facilitate accurate dosing. Administer with food to aid absorption. If intravenous treatment has been initiated, oral therapy should commence within 12 hours.
How long does treatment need to be continued after ingestion of an anticoagulant rodenticide?
As the anticoagulant effects of rodenticides are known to be long-lasting, it is recommended to administer Vitamivet K1® oral formulation for at least 3 weeks. The duration of treatment may be extended for as long as the anticoagulant persists in the body. Due to the availability of more potent second-generation anticoagulant rodenticides, a longer treatment duration may be required depending on the active ingredient involved. We recommend reassessing prothrombin time (PT) 48 hours after discontinuation to ensure coagulopathy does not recur. Clotting tests performed during vitamin K1 therapy may appear normal because treatment restores clotting factors and can therefore mask ongoing anticoagulant effects.
Is Vitamivet K1® injectable licensed for intravenous or subcutaneous use?
Vitamivet K1® injectable is licensed for intravenous use only in dogs. Administration via other routes, such as subcutaneous injection, would therefore be considered off-label.
Some references, including the BSAVA Formulary, describe subcutaneous use. Historically, vitamin K1 was not administered intravenously in dogs due to the risk of acute hypersensitivity (anaphylactoid) reactions. These reactions were associated with solubilising agents, particularly polyoxyethylated fatty acid derivatives such as Cremophor EL used in older formulations (e.g. Konakion). More recent formulations use alternative solubilisers (mixed micelles), which have been shown not to trigger these reactions in dogs. Vitamivet K1® does not contain Cremophor EL and is licensed for intravenous use, with administration recommended as a slow IV injection. Intravenous administration also provides more reliable absorption and faster correction of coagulopathy
What are the storage requirements of Vitamivet K1® injectable and tablets?
Vitamivet K1® solution for injection has an unopened shelf life of 3 years and should be used immediately after opening. Any solution remaining in the ampoule following withdrawal of the required dose should be discarded. Store below 25°C and protect from light.
Vitamivet K1® oral tablets have an unopened shelf life of 4 years. The shelf life of any divided tablets is 3 days. Keep the blister strip in the outer carton and protect it from light. Any remaining tablet portion should be given at the next administration.
When should prothrombin time be monitored after anticoagulant rodenticide exposure and vitamin K1 therapy?
Prothrombin time (PT) is usually the first coagulation parameter to become prolonged after anticoagulant rodenticide exposure, often within 48 hours, while clinical haemorrhage typically develops within 3-5 days. Where possible, a coagulation profile should ideally be performed before starting vitamin K1 therapy, as treatment can rapidly normalise clotting times and mask diagnosis. PT should be rechecked 48 hours after discontinuing vitamin K1 therapy to confirm that coagulopathy has not recurred.
What is the dose of Emedog®? Onset of effect?
When administered subcutaneously at the recommended dose (0.1 mg/kg), Emedog® induces vomiting within 2–15 minutes. It has a short elimination half-life of approximately 30 minutes and is completely eliminated from healthy dogs within 2.5–3 hours. Accurate dosing is essential to ensure effective emesis and avoid subtherapeutic responses.
What are the storage requirements of Emedog®?
Emedog® has an unopened shelf life of 4 years and should be used immediately after opening. Any solution remaining in the ampoule following withdrawal of the required dose should be discarded. Emedog® (apomorphine) is not a controlled drug and as such, does not have to be locked away, however it is good practice to store Emedog® somewhere that will be easy to access in an emergency, such as in an emergency box or cupboard. Emedog® should be stored in the original package, protected from light. It does not require storing in the fridge.
Should antiemetics routinely be given after Emedog®?
The use of anti-emetics, following apomorphine, can be considered as per Emedog’s® SPC 4.10 “Maropitant (or dopamine receptor antagonists such as metoclopramide) should be considered in cases of protracted vomiting”. However, this should be considered on a case-by-case basis.
We don’t recommend a blanket approach for the use of anti-emetics following Emedog®. In general, an anti-emetic is usually not required as apomorphine has a short half-life of ~ 30 minutes and is therefore eliminated by 2.5-3 hours. Anti-emetics such as maropitant or metoclopramide can take a while to reach therapeutic plasma concentrations, and by then, often the effects of Emedog® will be subsiding (particularly as you want to wait until the stomach has been adequately emptied to recover as much of the undesirable substance as possible). Antiemetics may prove useful if the case requires urgent medication or activated charcoal (Carbodote) following emesis. Before reaching for an anti-emetic, it’s worth considering whether the patient is likely to reoffend within 24-48 hours as repeat attempts to induce emesis may prove ineffective until the anti-emetic has been eliminated from the body.
Are there any age or weight restrictions for using Emedog®?
There are no age or weight restrictions. All patients should be weighed accurately to ensure correct dosing and monitored closely after administration of Emedog®
Can Emedog® be redosed?
According to the Emedog® SPC section 4.4, if emesis is not induced following a single injection, do not repeat the injection, as it will not be effective and may provoke clinical signs of toxicity.
If the patient has received Emedog® and re-ingests an undesirable substance on the same day, a repeat dose may be considered provided emesis is not contraindicated, the patient is conscious, and the gag reflex is present. The licensed dose may be repeated via the licensed route if 2.5–3 hours have elapsed since the initial Emedog® injection. Emedog® has a short half-life of approximately 30 minutes and, in healthy dogs, is completely eliminated within 2.5–3 hours after administration.
Can Emedog® be administered to cats?
Do not use Emedog® in cats or other non-target species. Emedog® contains apomorphine, which is licensed for dogs only. Apomorphine can cause CNS excitation and is unreliable as an emetic in cats.
Can Emedog® be administered to pregnant or lactating dogs?
The safety of Emedog® has not been established during pregnancy and lactation in dogs. Apomorphine has been shown to have teratogenic effects in rabbits and foetotoxic effects in rats at doses higher than the recommended dose in dogs. As apomorphine is excreted in breast milk, when used in lactating females, puppies should be monitored carefully for undesired effects. The decision to use Emedog® should be based on an individual risk: benefit assessment by the prescribing clinician
What is the onset of effect of Vitamivet K1® following intravenous or oral administration?
Following intravenous administration, Vitamivet K1® produces a rapid effect in dogs, with prothrombin time (PT) often normalising within a few hours. After oral administration, PT typically normalises within 12-24 hours, but may take up to 48 hours depending on the patient and factors affecting gastrointestinal absorption.
SPCs
Where can I find the Emedog SPC?
Where can I find the Vitamivet K1 Tablets SPC?
Where can I find the Vitamivet K1 Injection SPC?
Where can I find the Ziapam SPC?
Where can I find the Fluoxevet SPC?
Where can I find the Sileo SPC?
Where can I find the Tessie SPC?
Where can I find the Bonqat SPC?
Where can I find the Stromease SPC?
Where can I find the Soliphen SPCs?
You can find the Soliphen 15mg SPC on the VMD website here.
You can find the Soliphen 60mg SPC on the VMD website here.
You can find the Soliphen 120mg SPC on the VMD website here.
Where can I find the Vetbromide SPC?
Where can I find the Dogstem SPC?
Need a hand ? You’re in the right place
1. Lamminen T, Korpivaara M, Aspegrén J, Palestrini C, Overall KL. Pregabalin Alleviates Anxiety and Fear in Cats during Transportation and Veterinary Visits—A Clinical Field Study. Animals. 2023; 13(3):371.
TESSIE® 0.3 MG/ML ORAL SOLUTION FOR DOGS. Contains Tasipimidine. POM-V. For the short term alleviation of situational anxiety and fear in dogs triggered by noise or owner departure. BONQAT® 50 MG/ML ORAL SOLUTION FOR CATS contains Pregabalin. Schedule 3 POM-V . For the alleviation of acute anxiety and fear associated with transportation and veterinary visits. SILEO® 0.1 mg/ml oromucosal gel for dogs. Contain Dexmedetomidine hydrochloride. POM-V . For the alleviation of acute anxiety and fear associated with noise in dogs. FLUOXEVET 32MG TABLETS FOR DOGS contain fluoxetine. Legal category POM-V. As an aid in the treatment of separation-related disorders in dogs. Stromease® 25 mg/ml eye drops, solution for dogs and cats contains Acetylcysteine. Legal category POM-V. For the supportive treatment of corneal ulcers in dogs and cats. Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contraindications. DogStem is licensed for the improvement in function and reduction of pain and lameness associated with mild to severe osteoarthritis in hip and elbow joints. DogStem suspension for injection for dogs contains 6.5×106 – 9×106 equine umbilical cord mesenchymal stem cells. Legal category POM-V . Soliphen® 15mg, Soliphen® 60mg and Soliphen® 120mg tablets for oral use in dogs. Tablets contain phenobarbital and can be divided into halves and quarters for Soliphen® 60mg and 120mg, and into halves for Soliphen® 15mg Legal category POM-V CD Sch.3. For the prevention of seizures due to generalised epilepsy in dogs. Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contra-indications. Vetbromide® 600mg tablets for dogs contains potassium bromide. Legal category POM-V. An anti-epileptic agent for use in the control of idiopathic epileptic seizures, either as a single agent or adjunct to phenobarbital in the control of refractory cases of idiopathic epilepsy. Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contra-indications. Ziapam® 5mg/ml solution for injection for cats and dogs contains Diazepam. Legal category POM-V CD Sch.4 . In cats and dogs for the short-term management for convulsive disorders and skeletal muscle spasms of central and peripheral origin. As part of a pre-anaesthetic or sedation protocol. Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contra-indications. Emedog® 1 mg/ml, solution for injection for dogs contains Apomorphine. Legal category POM-V. For the induction of emesis in dogs. Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contra-indications. Vitamivet K1® TVM solution for injection for dogs, 10 mg/ml. Legal category POM-V . 1ml contains 10mg of Phytomenadione. Indications for use: In dogs: emergency treatment of anticoagulant rodenticide poisoning, before starting oral treatment. Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contraindications. Vitamivet K1® TVM 50 mg film-coated tablets for dogs. Legal category NFA-VPS . Contains 50mg of Phytomenadione. Indications for use: In dogs: Treatment of anticoagulant poisoning, following parenteral treatment Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contra-indications. Ziapam® 5mg/ml solution for injection for cats and dogs contains Diazepam. Legal category POM-V Sch. 4 CD . In cats and dogs for the short-term management for convulsive disorders and skeletal muscle spasms of central and peripheral origin. As part of a pre-anaesthetic or sedation protocol. Please refer to the product packaging and leaflets for information about side effects, precautions, warnings and contra-indications.® Registered trademarks of Dômes Pharma group companies.
Use Medicines Responsibly. www.noah.co.uk/responsible. Prescription decisions are for the person issuing the prescription alone.
BONQAT®, SILEO® and TESSIE® are developed and manufactured by Orion Corporation and distributed by TVM-UK Animal Health Ltd.
This information is intended for GB distribution only. For further information and to view the full Summary of Product Characteristics, please contact Dômes Pharma. Dômes Pharma is the trading name of TVM UK Animal Health Ltd, Kirtlington Business Centre, Slade Farm, Kirtlington, Oxfordshire, UK. OX5 3JA. 0800 0385868. www.domespharma.co.uk help@domespharma.com. ©2025 Orion Group. All rights reserved.